Overview
The appearance of flat feet is normal and common in infants, partly due to "baby fat" which masks the developing arch and partly because the arch has not yet fully developed. The human arch develops in infancy and early childhood as part of normal muscle, tendon, ligament and bone growth. Training of the feet, especially by foot gymnastics and going barefoot on varying terrain, can facilitate the formation of arches during childhood, with a developed arch occurring for most by the age of four to six years. Flat arches in children usually become proper arches and high arches while the child progresses through adolescence and into adulthood.
Causes
As discussed above, many health conditions can create a painful flatfoot. Damage to the posterior tibial tendon is the most common cause of AAFD. The posterior tibial tendon is one of the most important tendons of the leg. It starts at a muscle in the calf, travels down the inside of the lower leg and attaches to the bones on the inside of the foot. The main function of this tendon is to hold up the arch and support your foot when you walk. If the tendon becomes inflamed or torn, the arch will slowly collapse. Women and people over 40 are more likely to develop problems with the posterior tibial tendon. Other risk factors include obesity, diabetes, and hypertension. Having flat feet since childhood increases the risk of developing a tear in the posterior tibial tendon. In addition, people who are involved in high impact sports, such as basketball, tennis, or soccer, may have tears of the tendon from repetitive use.
Symptoms
The majority of children and adults with flexible flatfeet never have symptoms. However, their toes may tend to point outward as they walk, a condition called out-toeing. A person who develops symptoms usually complains of tired, aching feet, especially after prolonged standing or walking. Symptoms of rigid flatfoot vary depending on the cause of the foot problem. Congenital vertical talus. The foot of a newborn with congenital vertical talus typically has a convex rocker-bottom shape. This is sometimes combined with an actual fold in the middle of the foot. The rare person who is diagnosed at an older age often has a "peg-leg" gait, poor balance and heavy calluses on the soles where the arch would normally be. If a child with congenital vertical talus has a genetic disorder, additional symptoms often are seen in other parts of the body. Tarsal coalition. Many people have no symptoms, and the condition is discovered only by chance when an X-ray of the foot is obtained for some other problem. When symptoms occur, there is usually foot pain that begins at the outside rear of the foot. The pain tends to spread upward to the outer ankle and to the outside portion of the lower leg. Symptoms usually start during a child's teenage years and are aggravated by playing sports or walking on uneven ground. In some cases, the condition is discovered when a child is evaluated for unusually frequent ankle sprains. Lateral subtalar dislocation. Because this often is caused by a traumatic, high-impact injury, the foot may be significantly swollen and deformed. There also may be an open wound with bruising and bleeding.
Diagnosis
You can always give yourself the ?wet test? described above to see whether you have flat feet. Most people who do not notice their flat feet or have no pain associated with them do not think to see a foot doctor. Flat feet can lead to additional problems such as stiffness or pain, however, especially if the condition appears out of nowhere. If you think you may have flat feet, you should seek medical attention to ensure there are no additional issues to worry about. Your doctor will be able to diagnose you with a number of tests. For example, he or she may have you walk around, stand still, or stand on your tiptoes while you are being examined. Your doctor may also examine your foot?s shape and functionality. It?s important to let your foot doctor know about your medical and family history. In some cases, your doctor may order imaging tests such as x-rays or an MRI (magnetic resonance imaging) to determine a cause of your flat foot. If tarsal coalition is suspected in children, a CT scan is often ordered.
pes planus exercises
Non Surgical Treatment
Orthotics. Interpod orthotics re-align and support the foot; therefore reducing any excessive stress when walking or during activity. Orthotics can assist with maintaining arch profile and allow for more effective functioning of joints. Footwear. A strong supportive, well fitted shoe may assist with reducing excessive pronation and support the joints of your feet. A supportive shoe will also help maximise the function of your Interpod orthotic. Padding may be applied to your shoes or feet by your practitioner to reduce excessive stress. Specific taping techniques can be applied by your practitioner to improve foot function. Your practitioner may advise certain stretches or exercises to assist with maintaining foot function and reduce painful symptoms. Pain medication such as NSAIDs (ibuprofen) may be advised by your practitioner. If all conservative options have been exhausted, then surgical correction of flat feet may be undertaken.
Surgical Treatment

Rarely does the physician use surgery to correct a foot that is congenitally flat, which typically does not cause pain. If the patient has a fallen arch that is painful, though, the foot and ankle physicians at Midwest Orthopaedics at Rush may perform surgery to reconstruct the tendon and "lift up" the fallen arch. This requires a combination of tendon re-routing procedures, ligament repairs, and bone cutting or fusion procedures.
The appearance of flat feet is normal and common in infants, partly due to "baby fat" which masks the developing arch and partly because the arch has not yet fully developed. The human arch develops in infancy and early childhood as part of normal muscle, tendon, ligament and bone growth. Training of the feet, especially by foot gymnastics and going barefoot on varying terrain, can facilitate the formation of arches during childhood, with a developed arch occurring for most by the age of four to six years. Flat arches in children usually become proper arches and high arches while the child progresses through adolescence and into adulthood.
Causes
As discussed above, many health conditions can create a painful flatfoot. Damage to the posterior tibial tendon is the most common cause of AAFD. The posterior tibial tendon is one of the most important tendons of the leg. It starts at a muscle in the calf, travels down the inside of the lower leg and attaches to the bones on the inside of the foot. The main function of this tendon is to hold up the arch and support your foot when you walk. If the tendon becomes inflamed or torn, the arch will slowly collapse. Women and people over 40 are more likely to develop problems with the posterior tibial tendon. Other risk factors include obesity, diabetes, and hypertension. Having flat feet since childhood increases the risk of developing a tear in the posterior tibial tendon. In addition, people who are involved in high impact sports, such as basketball, tennis, or soccer, may have tears of the tendon from repetitive use.
Symptoms
The majority of children and adults with flexible flatfeet never have symptoms. However, their toes may tend to point outward as they walk, a condition called out-toeing. A person who develops symptoms usually complains of tired, aching feet, especially after prolonged standing or walking. Symptoms of rigid flatfoot vary depending on the cause of the foot problem. Congenital vertical talus. The foot of a newborn with congenital vertical talus typically has a convex rocker-bottom shape. This is sometimes combined with an actual fold in the middle of the foot. The rare person who is diagnosed at an older age often has a "peg-leg" gait, poor balance and heavy calluses on the soles where the arch would normally be. If a child with congenital vertical talus has a genetic disorder, additional symptoms often are seen in other parts of the body. Tarsal coalition. Many people have no symptoms, and the condition is discovered only by chance when an X-ray of the foot is obtained for some other problem. When symptoms occur, there is usually foot pain that begins at the outside rear of the foot. The pain tends to spread upward to the outer ankle and to the outside portion of the lower leg. Symptoms usually start during a child's teenage years and are aggravated by playing sports or walking on uneven ground. In some cases, the condition is discovered when a child is evaluated for unusually frequent ankle sprains. Lateral subtalar dislocation. Because this often is caused by a traumatic, high-impact injury, the foot may be significantly swollen and deformed. There also may be an open wound with bruising and bleeding.
Diagnosis
You can always give yourself the ?wet test? described above to see whether you have flat feet. Most people who do not notice their flat feet or have no pain associated with them do not think to see a foot doctor. Flat feet can lead to additional problems such as stiffness or pain, however, especially if the condition appears out of nowhere. If you think you may have flat feet, you should seek medical attention to ensure there are no additional issues to worry about. Your doctor will be able to diagnose you with a number of tests. For example, he or she may have you walk around, stand still, or stand on your tiptoes while you are being examined. Your doctor may also examine your foot?s shape and functionality. It?s important to let your foot doctor know about your medical and family history. In some cases, your doctor may order imaging tests such as x-rays or an MRI (magnetic resonance imaging) to determine a cause of your flat foot. If tarsal coalition is suspected in children, a CT scan is often ordered.
pes planus exercises
Non Surgical Treatment
Orthotics. Interpod orthotics re-align and support the foot; therefore reducing any excessive stress when walking or during activity. Orthotics can assist with maintaining arch profile and allow for more effective functioning of joints. Footwear. A strong supportive, well fitted shoe may assist with reducing excessive pronation and support the joints of your feet. A supportive shoe will also help maximise the function of your Interpod orthotic. Padding may be applied to your shoes or feet by your practitioner to reduce excessive stress. Specific taping techniques can be applied by your practitioner to improve foot function. Your practitioner may advise certain stretches or exercises to assist with maintaining foot function and reduce painful symptoms. Pain medication such as NSAIDs (ibuprofen) may be advised by your practitioner. If all conservative options have been exhausted, then surgical correction of flat feet may be undertaken.
Surgical Treatment
Rarely does the physician use surgery to correct a foot that is congenitally flat, which typically does not cause pain. If the patient has a fallen arch that is painful, though, the foot and ankle physicians at Midwest Orthopaedics at Rush may perform surgery to reconstruct the tendon and "lift up" the fallen arch. This requires a combination of tendon re-routing procedures, ligament repairs, and bone cutting or fusion procedures.




 If you sometimes feel that you are "walking on a marble," and you have persistent pain in the ball of your foot, you may have a condition called Morton's neuroma. A neuroma is a benign tumor of a nerve. Morton's neuroma is not actually a tumor, but a thickening of the tissue that surrounds the digital nerve leading to the toes. Morton's neuroma occurs as the nerve passes under the ligament connecting the toe bones (metatarsals) in the forefoot. Morton's neuroma most frequently develops between the third and fourth toes, usually in response to irritation, trauma or excessive pressure. The incidence of Morton's neuroma is 8 to 10 times greater in women than in men.
If you sometimes feel that you are "walking on a marble," and you have persistent pain in the ball of your foot, you may have a condition called Morton's neuroma. A neuroma is a benign tumor of a nerve. Morton's neuroma is not actually a tumor, but a thickening of the tissue that surrounds the digital nerve leading to the toes. Morton's neuroma occurs as the nerve passes under the ligament connecting the toe bones (metatarsals) in the forefoot. Morton's neuroma most frequently develops between the third and fourth toes, usually in response to irritation, trauma or excessive pressure. The incidence of Morton's neuroma is 8 to 10 times greater in women than in men.






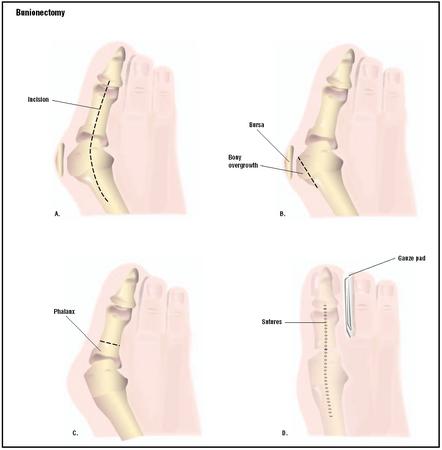 A bunion is a deformity of the metatarsophalangeal (MTP) joint at the base of the big toe. A bunion develops when the first metatarsal bone of the foot turns outward and the big toe points inward (toward the other toes), causing the joint to jut out. A bunion is most likely to develop when susceptible feet are repeatedly squeezed into narrow, pointed-toe footwear. The big toe pushes against the other toes, sometimes diving over or under them. As a result, the base of the big toe ? the metatarsophalangeal (MTP) joint ? juts or angles out from the foot.
A bunion is a deformity of the metatarsophalangeal (MTP) joint at the base of the big toe. A bunion develops when the first metatarsal bone of the foot turns outward and the big toe points inward (toward the other toes), causing the joint to jut out. A bunion is most likely to develop when susceptible feet are repeatedly squeezed into narrow, pointed-toe footwear. The big toe pushes against the other toes, sometimes diving over or under them. As a result, the base of the big toe ? the metatarsophalangeal (MTP) joint ? juts or angles out from the foot.
 The Achilles tendon is the tough sinew that attaches the calf muscle to the back of the calcaneus, or heel bone. It is also known as the tendo calcaneus or the tendo Achilles and happens to be one of the longest tendons in the body. An Achilles tendon rupture occurs when the Achilles tendon is partially or completely broken or torn. The average age of patients who suffer Achilles tendon ruptures is 30 to 40 years. The male-to-female ratio is nearly 20 to 1.
The Achilles tendon is the tough sinew that attaches the calf muscle to the back of the calcaneus, or heel bone. It is also known as the tendo calcaneus or the tendo Achilles and happens to be one of the longest tendons in the body. An Achilles tendon rupture occurs when the Achilles tendon is partially or completely broken or torn. The average age of patients who suffer Achilles tendon ruptures is 30 to 40 years. The male-to-female ratio is nearly 20 to 1.
